
Nothing Was Wrong Except the Complete Absence of Joy
High-functioning depression hides inside lives that are objectively successful.


This is an abridged version If you want the expanded version, it’s free here and includes more research, more personal narrative, and enough clinically precise oversharing to make at least one former professor briefly remove their glasses and stare at a wall.
I was thirty-two, running for city council in the third largest city in Indiana with no political experience.
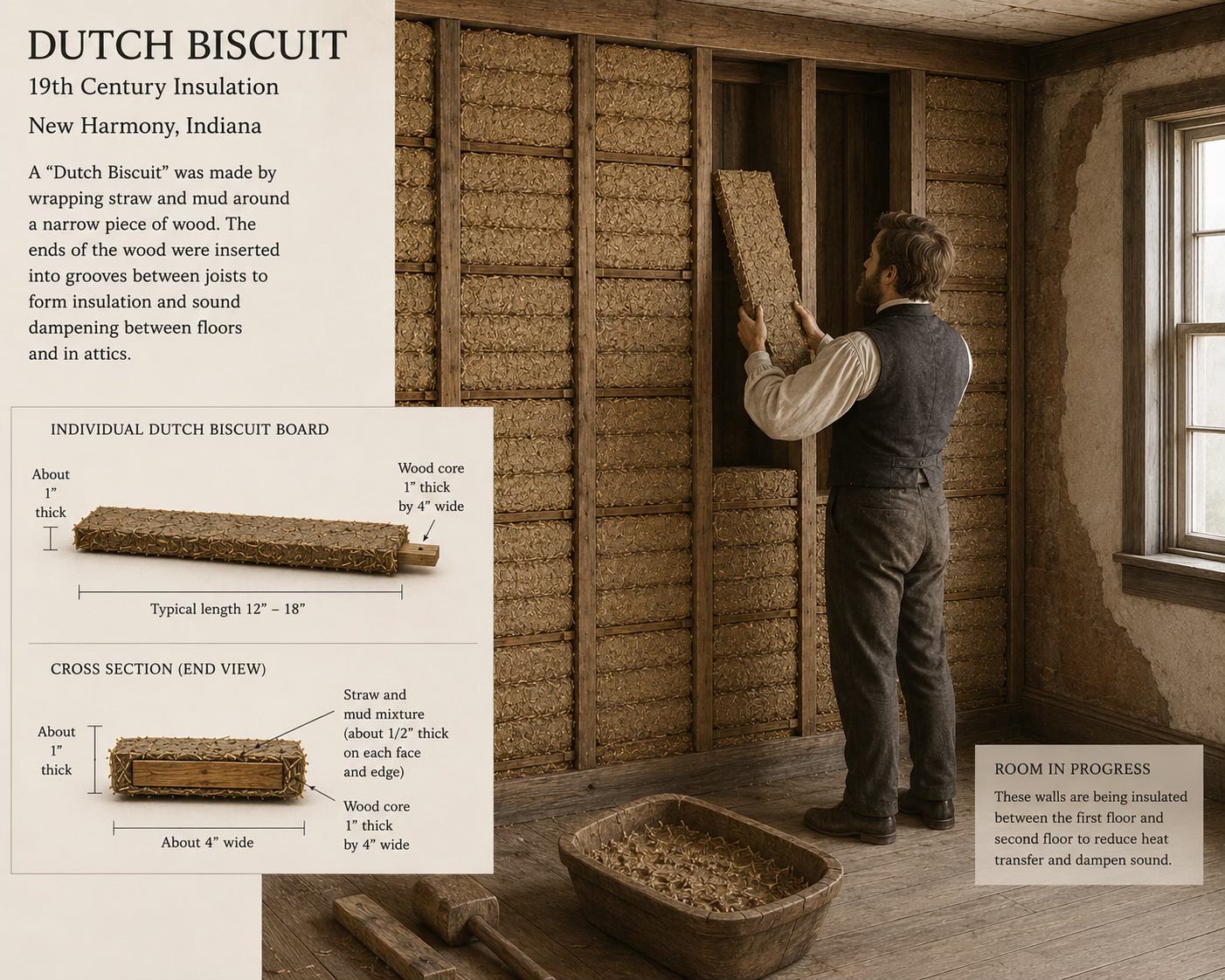
I was also pastoring a church and giving tours of a historic town where I enthusiastically explained how the bricks known as Dutch biscuits were made in the 1800s. Also I was getting divorced.
My whole life looked like a dare.
Every morning I woke up in the new house, stretched, ran, fed my dog, showered, put on my makeup, did my hair, and drove thirty minutes to the historic town. On the drive I noticed the height of the corn, the blue of the sky, and thought about driving my car into a tree1.
I never moved my steering wheel. But every day I glanced at the same tree and wondered if I could just be done. The rest of my day I shook hands, kissed babies, and performed enthusiasm about 19th century utopias for people who were mostly there because their spouses had insisted.
I was so depressed. And nobody knew. Including me.
High Functioning Depression
High-functioning depression is not a DSM diagnosis, but those who have it know what it is. It’s depression with a cute sparkle veneer. You meet your deadlines. You respond to texts. You train for marathons. You run for city council with no political experience and win.
The difference between this version and the version where you consider throwing all your dishes away in lieu of washing them is architectural.
In melancholic depression, the version nobody misses, the reward system and the cognitive system fail together. Working memory, problem-solving, executive function — measurably worse across the board (Zaninotto et al., 2016).
In high-functioning depression, the reward system gets blunted while the executive system keeps running. The ventral striatum, the part responsible for processing reward, reduces output (Pizzagalli, 2014). Nothing feels like much before you do it or after. But your prefrontal cortex is still planning, executing, managing a calendar that would hospitalize a person with normal energy reserves.
You learned early that collapse is not socially survivable, so you built workarounds. You overschedule. You intellectualize. You get very funny. You become a perfectionist, because if you’re doing everything right, nobody looks too closely. And when nobody looks too closely, nobody has to wonder if the sad depressed girl is capable of managing the city.
This perfectionism is a pleasure-starved brain recalibrating around whatever still produces a signal. Achievement becomes one of the few things that reliably gives you any feeling at all.
Socially prescribed perfectionism is the belief that other people require your flawlessness and it will encourage you to withdraw if your imperfection shows. It has the strongest association with depression and, critically, with concealment (Hewitt et al., 2017). You’re doing everything right so nobody asks how you’re doing.
The depression blunts the reward system. The blunted reward system makes achievement one of your only functioning sources of relief. Achievement requires performance. Performance requires concealment. Concealment prevents anyone from identifying that you’re depressed. Including you. It is an infinity loop straight from hell and it runs so quietly you don’t notice it at all.
One Reason > Thirteen
I have long been a great fan of doorknobing my therapist. Doorknobing is the art and science of slamming your therapist with a big issue three minutes before the end of session, while your hand is on the doorknob, so you won’t have to deal with the fallout of what you just said.
Oh, by the way, I’m having an affair. Also I’ve been taking private loans from someone I met online. We’ll put a pin in that for next week.
On one Tuesday afternoon I decided I was finally going to tell my therapist that I had been seeing trees on my drive to work. I carefully watched the clock until I had three minutes left. I’mthinkingaboutkillingmyself, I said in a rush. I expected him to reach for his phone. The serious phone call. The inpatient unit.
What he asked instead was: why haven’t you done it?
I said I don’t want my dog to miss me.
He said that was one reason and it was enough.
He wasn’t being glib. One protective factor is sufficient for people to want to continue to live (Linehan et al., 1983). The threshold is that low. It doesn’t have to be a person. It doesn’t have to be proportionate to the pain or make sense to anyone else.
My reason was Olga Jeanette, an aging terrier with the personality of a retired dock worker and the unwavering belief that I am God’s greatest achievement. If I didn’t come home, she would wait by the door. She would have no way of being told, of understanding why I abandoned her.
One was and is enough.

What I had described that day to my therapist was passive ideation, the clinical term for thoughts of suicide without intent or plan. It is also almost never said out loud. The people experiencing it know it sounds alarming. They also know they are not going to act on it and they don’t want to be hospitalized. About 9% of the general population will experience passive ideation at some point; in people with depression, the number is considerably higher (Nock et al., 2008).
Most of them say nothing. Most of them just keep an eye on a particular tree.
Just Because You Went to Medical School…
My therapist told me it was time to talk to my doctor about medication. He knew that being depressed is fucking miserable and I would absolutely white-knuckle my way through it. He also knew I didn’t have to live that way.
I took his advice and made an appointment. My doctor told me to keep an anxiety journal.
I had driven to that appointment from a marriage that was ending, handed him a referral from a therapist who had explicitly sent me for medication, and described thoughts about driving into a tree. He offered me a blank notebook. When I explained that I’d been in therapy for ten years and I’d be happy to hand him an anxiety encyclopedia organized by the worst thing I had done or by year according to his preference, he agreed to try medication.
He chose trazodone, which is primarily a sleep aid that developed antidepressant aspirations at some point in its clinical career. It is used off-label for mild-to-moderate depression. It is not the standard-of-care response to passive suicidal ideation.
He prescribed it because I presented well. I walked in with complete sentences, done hair, makeup, and a blazer and he concluded, from this evidence, that I was probably fine.
This is the biggest problem with high-functioning depression. Because you present well, because you are so accustomed to the feeling of being down that it registers as baseline, the standard depression screenings often miss you. The more together you look, the less aggressively you get treated.
If you are in a clinical setting and being handed something inadequate, you are allowed to say so. My therapist specifically referred me for an SSRI and I’d like to understand why you chose differently works. I wish I had known enough at the time to advocate for myself.
How to Fix It
This section is the most abridged, if you’re interested in how to work with high-functioning depression the full essay contains it all. Read it free here.
Chronic depression running on elevated cortisol for years physically shrinks your hippocampus — the part of your brain responsible for memory, learning, and emotional regulation gets measurably smaller the longer depression goes untreated (Duman et al., 2000). Antidepressants reverse that process by increasing BDNF, brain-derived neurotrophic factor, which promotes the growth of new neurons and measurable structural recovery (Castrén & Hen, 2013). SSRIs can potentially reverse structural damage that has been accumulating the entire time you were explaining 19th century bricks.
Treatment is not self-indulgent. It is the most logical response to structural damage that has been accumulating while you were busy proving you were okay.
You were never fine. You were just very good at not being fine, and those are not the same thing.
It Changes.
The tour group on that Tuesday in October tipped well. They thanked me. A woman in a yellow rain jacket said I was the best guide she’d ever had.
I drove home and felt nothing, and then I drove home again the next day, and the day after that, for years, and the whole time I was the best guide anyone had ever had. I won the council seat. I gave excellent sermons. I was, by every available metric, doing great.
The tree is still on that road. I drove past it for six month before I told anyone it was there.
The thing about high-functioning depression is that it doesn’t end dramatically. Nobody stages an intervention. Nobody “finds” you. You just eventually get tired enough of your own performance that you say something, usually at the last possible second, usually with your hand on a doorknob. And then someone asks the right question, and you say something about a dog, and that’s enough.
Olga Jeanette is thirteen years old now. I remind her every day that she’s my best friend and she accepts this as obvious. There is also now a husband, a step-kid, a second dog named Edward Scissorface, and a foster cat I refuse to call anything other than Cat, because naming her would mean admitting something.

You find new reasons. That’s the assignment. The first one was a terrier who moved through life like she had already filed three complaints that morning and believed I was destined for greatness, and she held the whole thing together without knowing she was doing it.
The reasons accumulate.
You stop counting them and start just living inside them. That’s how you know it’s working.
—
If you are experiencing thoughts of suicide or passive suicidal ideation, the 988 Suicide and Crisis Lifeline is available 24/7 by call or text. If you are looking for a therapist who specializes in persistent depressive disorder, the Psychology Today directory at psychologytoday.com allows filtering by specialty and insurance.
Further Reading
The Noonday Demon by Andrew Solomon. Solomon wrote this after his own severe depression, which means 600 pages on the biology, culture, politics, economics, and pharmaceuticals of the illness reads like dispatches from the inside rather than clinical summary from a comfortable distance. It is particularly strong on what chronic low-grade depression costs across a lifetime, which is the part most books skip entirely. It will take you a while. It will be worth it.
Why People Die by Suicide by Thomas Joiner. Joiner developed the interpersonal theory of suicide after his own father died by suicide, so this is not abstract theorizing from a comfortable professional distance. The framework he builds, around thwarted belonging and perceived burdensomeness, is the most clinically useful language I have found for why one reason to stay is enough. The title is doing the hardest possible marketing work for what is, genuinely, a hopeful book.
Good Reasons for Bad Feelings by Randolph Nesse. Nesse is an evolutionary psychiatrist who argues that your symptoms exist for a reason, and that treating them without understanding the function is how you end up disabling the smoke alarm instead of finding the fire. Useful if you have spent years wondering why you’re depressed when nothing is technically wrong, or if you have quietly decided that your depression is just accurate perception of how the world works. Nesse will complicate that.
Perfectly Hidden Depression by Margaret Robinson Rutherford. Rutherford spent decades watching the same person walk into her office: high-functioning, accomplished, visibly fine, privately not. This book is written for that person, which means it is written for the person who read this essay and thought “yes, but I’m probably not depressed enough to count.” It covers the perfectionism-concealment-depression loop in plain language, includes exercises, and has the specific quality of making you feel caught rather than informed.
The Upward Spiral by Alex Korb. Korb is a neuroscientist who writes about depression the way this newsletter tries to: evidence-based, mechanistic, and actually readable. Where most neuroscience writing makes you feel like you’re being explained at, this one explains the brain circuitry of depression and then tells you what to do about it, in the same breath. Useful if the neuroscience sections of this essay made you want more and reading a clinical paper sounds like homework.
As an Amazon Associate I earn from qualifying purchases, though your purchase costs the same either way. Honestly, if your local library has the book, start there. Libraries remain one of humanity’s better ideas.
—
Works Cited
Castrén, E., & Hen, R. (2013). Neuronal plasticity and antidepressant actions. Trends in Neurosciences, 36(5), 259–267. https://doi.org/10.1016/j.tins.2012.12.010
Duman, R. S., Malberg, J., Nakagawa, S., & D’Sa, C. (2000). Neuronal plasticity and survival in mood disorders. Biological Psychiatry, 48(8), 732–739. https://doi.org/10.1016/S0006-3223(00)00935-5
Hewitt, P. L., Flett, G. L., & Mikail, S. F. (2017). Perfectionism: A relational approach to conceptualization, assessment, and treatment. Guilford Press.
Klein, D. N. (2010). Chronic depression: Diagnosis and classification. Current Directions in Psychological Science, 19(2), 96–100. https://www.jstor.org/stable/41038548
Linehan, M. M., Goodstein, J. L., Nielsen, S. L., & Chiles, J. A. (1983). Reasons for staying alive when you are thinking of killing yourself: The Reasons for Living Inventory. Journal of Consulting and Clinical Psychology, 51(2), 276–286. https://doi.org/10.1037/0022-006X.51.2.276
Nock, M. K., Borges, G., Bromet, E. J., Alonso, J., Angermeyer, M., Beautrais, A., Bruffaerts, R., Chiu, W. T., de Girolamo, G., Gluzman, S., de Graaf, R., Gureje, O., Haro, J. M., Huang, Y., Karam, E., Kessler, R. C., Lepine, J. P., Levinson, D., Medina-Mora, M. E., … Williams, D. (2008). Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. British Journal of Psychiatry, 192(2), 98–105. https://doi.org/10.1192/bjp.bp.107.040113
Pizzagalli, D. A. (2014). Depression, stress, and anhedonia: Toward a synthesis and integrated model. Annual Review of Clinical Psychology, 10, 393–423. https://doi.org/10.1146/annurev-clinpsy-050212-185606
Zaninotto, L., Solmi, M., Veronese, N., Guglielmo, R., Ioime, L., Camardese, G., & Serretti, A. (2016). A meta-analysis of cognitive performance in melancholic versus non-melancholic unipolar depression. Journal of Affective Disorders, 201, 15–24. https://doi.org/10.1016/j.jad.2016.04.039

I share this story with a tiny bit of fear but zero shame. I share it with people in my life, with clients, with people reading my blog. A friend going through his own divorce would call me on a hard day and say, Kaitlin, I’m seeing trees. He went on to fall in love again, get engaged, get happy, and then get cancer and fight like hell. People probably don’t want to die as much as the moment says they do.